
The MMR vaccine for Measles, Mumps, and Rubella is a HOT topic with lots of angles to explore. The vaccine itself is designed to prevent three distinct illnesses, but MEASLES tends to get most of the headlines and media attention, especially right now as outbreaks are making the headlines and legislation for government mandated vaccines comes down the pipe in many states.
Throughout my research on all three illnesses, there was a noticeable disconnect between the fearful and emergency-like undertones from the mainstream media and what I learned from reading actual primary resources (along with talking to mine and my husband’s grandparents who both went through these childhood illnesses with their children and as children themselves.)
Then there’s this video showing the Brady Bunch kids in the 60’s laughing and joking about having the measles in contrast to a current-day Law and Order SVU episode where they declare a measles state of emergency. It’s seriously baffling. Stop everything and watch it before you read on.
I originally discussed all three MMR diseases in this post but decided after writing such a lengthy amount about measles that I was going to break them into two with an additional post on the MMR alone. You can find the other parts of the MMR in the Mumps and Rubella portion in Part 8 and read the data, ingredients concerns, alternative vaccine schedules, and more about the possible autism link in my next post on the MMR.
This is Part 7 in my vaccine series discussing which vaccines we decided to give to our children and why. You may also want to check out the other posts in this series:
Part 1: Our Vaccine Choice: Risks, Benefits, Responsibility
Part 2: Hepatitis B and Hib Vaccines
Part 3: Diphtheria, Tetanus and Pertussis Vaccine
Measles Basics:
Overview (CDC)
Before the measles vaccination program started in 1963, an estimated 3 to 4 million people developed measles infection each year in the United States (although only ~500,000 were reported each year to the CDC.) Approximately 400-500 people died each year from complications with measles in the U.S prior to the vaccine (about 0.2 out of every 100,000 people.)
- Measles is a contagious viral infection characterized by high fever and bodily rash.
- Measles is spread through respiratory particles (sneezing, coughing, etc.)
- Rash begins on average 14 days after initial exposure.
- Measles may be transmitted from 4 days before to 4 days after rash onset. It is most contagious from onset of fever through the first 3–4 days of rash.
- Before the vaccine, children ages 5-9 were the most common group to get measles and approximately 90% of Americans had immunity by age 15 through natural infection.
- Since the measles vaccine has been around for several generations, measles complication risk has shifted to adults and the very young (since vaccinated mothers do not have the same antibody protection as naturally exposed mothers- see population studies from the 1980’s further down in this post).
- Malnutrition and overall wellness of the child will affect severity of symptoms (One of many sources showing this.)
Measles Symptoms:
- High fever (103-105 degrees Fahrenheit)
- Cough
- Runny nose
- Flat, red (itchy) rash that lasts 5-6 days beginning at the hairline and working its way down to the feet and arms. It recedes in the same order it appears.
- Loss of appetite
- conjunctivitis (red, watery eyes) with sensitivity to light
- Koplic spots (white spots present in the mucous membranes such as the mouth) may occur 1-2 days before typical measles rash.
- Complications from measles (mostly in children under 5): diarrhea (8% of cases), ear infections (7% of cases), pneumonia (6% of cases- most measles deaths occur from pneumonia so knowledge of care is essential- see below), acute encephalitis (0.1% of cases), seizures (0.6-0.7% of cases.)
- This group of measles case studies from Johns Hopkins in 1957 gives us an excellent idea of what measles complications and their longterm outcomes looked like before the vaccine. This also varies greatly depending on the nutrition and nourishment of the population, especially with Vitamin A deficiency.
Making Decisions Based on Measles Statistics:
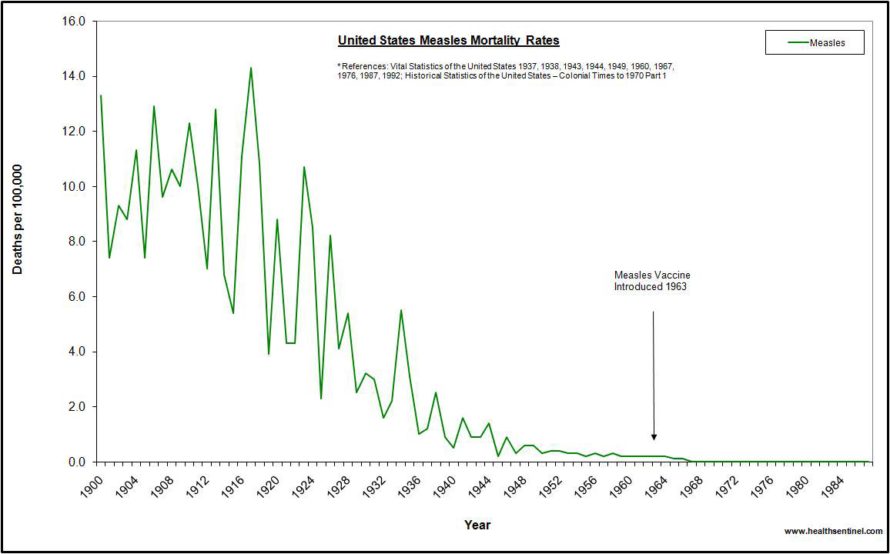
You can find the complete list of these statistics used for this graph HERE. (Thank you to Dr. Suzanne Humphries and Roman Bystrianyk for compiling this graph.)
In the late 1800’s and early 20th century we saw a significant decrease in ALL diseases, most BEFORE the vaccine era. Public sanitation improvements such as water treatment, indoor plumbing (solid waste disposal,) regulations on overcrowded housing, and public programs for improved nutrition and health departments, were SIGNIFICANT in this improvement. Also- proper disposal of animal feces and animal control were addressed in the early 20th century along with trash service and hand washing campaigns.
Many diseases such as scarlet fever, cholera, dysentery, tuberculosis, yellow fever and typhoid fever didn’t have a vaccine at all (or their vaccine was never widely used) and we rarely see these diseases today in developed areas. You can see some graphs depicting this HERE.
The fact is that in 1962, the year before the vaccine was introduced, measles killed 0.2 of everyone 100,000 people in the U.S. (which for the population of 189,000,000 at the time was 408 people).
Compare this to Influenza/ Pneumonia which killed 32.3 per 100,000 (~60,000) people and cancer which killed 150 per every 100,000 (~283,000) people. Heart disease killed 400 per 100,000 (~750,000) people! Source: MMWR Annual Report, 1963
In 1963, the year the vaccine was introduced (although it didn’t become widely used until the late 60’s,) there were 363 deaths from measles. Meanwhile, over 43,000 people died in car accidents and over 700,000 people died from heart disease. You were much more likely to be one of the 9,200 people murdered in that year than to die from measles. And lastly- over 20,000 children died from congenital defects, 46 times more than died from measles. Source: MMWR Annual Report, 1964
0.2 out of every 100,000 is a significantly low chance of dying from measles. That means if I get measles tomorrow, I have a 1 in 10,000 chance of dying. Of course it saddens me to hear of anyone dying from anything, but today I get upset when I hear that over 250,000 people each year die from medical errors and 72,000 people die from pharmaceutical drug misuse and yet we get dramatic reports of measles outbreaks where no one died as headline news.
If these pre-vaccine numbers were translated to today’s population of 327 million, we would see ~1,000 deaths per year from the measles (although I imagine this would be slightly higher due to the vaccine shifting measles vulnerability – see below.)
There have been no confirmed deaths from measles in almost 20 years in the U.S. except for one woman in 2015 who, according to the Washington Department of Health, “had several other health conditions and was on medications that contributed to a suppressed immune system. She didn’t have some of the common symptoms of measles such as a rash, so the infection wasn’t discovered until after her death. The cause of death was pneumonia due to measles.”
There apparently have been 10 deaths from measles reported on death certificates in the U.S. since 2000, but none of these were confirmed and were considered questionable enough that they have not been included in the CDC mortality statistics.
Measles Vulnerability Has Shifted Due to the MMR:
Most of the complications we have seen in the last 30 years from measles have been because the vaccine has shifted the age of measles vulnerability towards adulthood when vaccine immunity has worn off, or in young babies that are too young to get the vaccine. This makes them vulnerable because their unvaccinated mothers do not have antibodies from natural measles immunity to pass on to them. It is true that in post-MMR outbreaks from the 1980’s and 1990’s deaths HAVE occurred in as frequent as 1 in 1,000 cases because of this shift in vulnerability.
Some doctors also noted that a large percentage of populations where outbreaks occurred were urban areas dealing with poverty and overcrowding and nutrition was a factor (in both Europe and the U.S.)
From the CDC pink book:
During the 1989–1991 measles resurgence, incidence rates for infants were more than twice as high as those in any other age group. The mothers of many infants who developed measles were young, and their measles immunity was most often due to vaccination rather than infection with wild virus. As a result, a smaller amount of antibody was transferred across the placenta to the fetus, compared with antibody transfer from mothers who had higher antibody titers resulting from wild-virus infection. The lower quantity of antibody resulted in immunity that waned more rapidly, making infants susceptible at a younger age than in the past.”
I found this really interesting newspaper clipping from a 1992 North Carolina newspaper on the “new problem” of babies getting measles dangerously earlier in life than their mothers did because their mothers were the first generation to have been vaccinated and lacked natural immunity.
The CDC’s conclusion? We just need to vaccinate these babies earlier, driving the move in the early 90’s from a 15-month-old MMR to a 12-month MMR. There have even been talks recently about moving it up to 9 months. This outbreak is also the reason why a second MMR was added to the schedule at 4-5 years as a booster even though measles incidence was already significantly low (and death was extremely rare.)
You can read the abstract of studies comparing antibody immunity titers of unvaccinated mothers to vaccinated mothers here:
Passive Immunity Against Measles During the First 8 Months of Life
Measles Antibodies in Women and Infants in the Vaccine Era
“The course of rubeola (measles) is benign and the patient’s recovery rapid.”
– Dr. H. Richard Tyler, MD, The Department of Neurology and Pediatrics, Johns Hopkins University, 1957
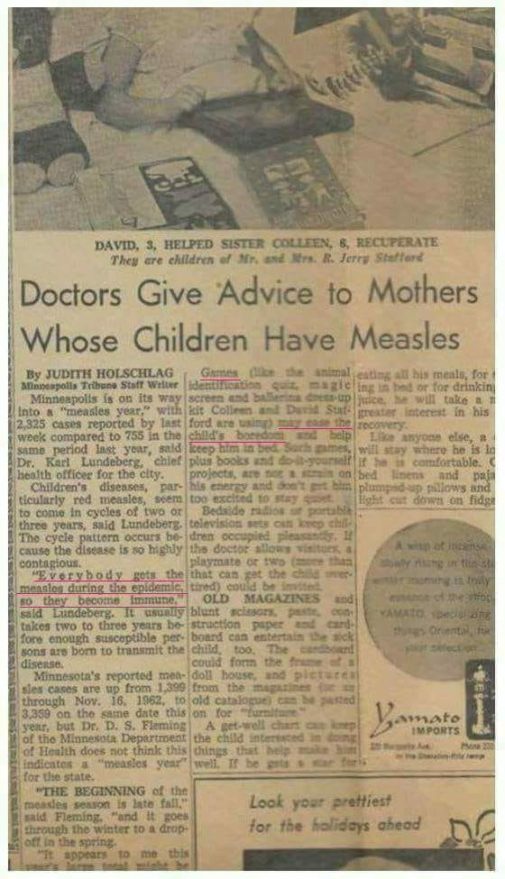
Minneapolis newspaper article from the 1950’s discussing how to entertain a child home with the measles.
Management and At Home Care for Measles:
Two generations ago, parents would have been very knowledgeable about how to care for children with measles and many other childhood illness at home. (You can see my conversations with my own grandmother below.) Today we are taught to take children to the doctor for even the most basic maladies and measles would be treated as an absolute emergency. But it doesn’t have to be this way. Here is a rundown of at-home care for measles:
- At first sign of respiratory congestion, runny nose, or cough, begin basic home care and keep children home from school and public places. Measles is most contagious once the fever occurs but can be spread through sneezing and coughing before then.
- Have children lay down and rest and allow fever to stay unless they become uncomfortably restless/ in pain or it rises above 104 degrees. Homeopathic remedies such as Belladonna can be used to bring the fever down to a safer, more comfortable level but will not interfere with the fever process of fighting the virus as giving ibuprofen would. You can read about that and additional homeopathy uses for measles HERE.
- In cases of stubborn fever above 104 degrees that won’t come down with homeopathy, a warm bath, wet sock hydrotherapy, or a cool washcloth on the forehead can be tried. (Take note that studies have shown that it is important for a positive measles outcome to avoid giving fever reducers such as ibuprofen and aspirin as long as possible. However, if my child’s fever gets over 104 or they are in pain and the above ideas aren’t working, I may consider giving a dye-free ibuprofen in a smaller dose to bring it down just a few degrees to comfort so they can rest.)
- Morbillinum (Morb) 30C is the homeopathic prophylactic used for measles to reduce symptoms and longevity. (There are many other remedies found in The Unvaccinated Child: A Treatment Guide for Parents and Caregivers.)
- Hydration is essential. Give water or an electrolyte lemonade (add 1/8 tsp Celtic sea salt to this recipe – electrolytes are especially important if diarrhea is present.)
- Basic nutritional support includes homemade bone broth, immune boosting and antiviral supplements such as ACF, a daily probiotic, garlic and garlic socks, and antiviral herbs such as elderberry syrup, astragalus, osha, and echinacea glycerides.
- Consider a 100,000-200,000 iu Vitamin A protocol under supervision of a holistic practitioner. Cod liver oil is a good source.
- German chamomile essential oil has antiviral properties and that along with lavender soothes rash and itching.
- To avoid respiratory complication it is important to keep nasal passages clear. Use a nasal irrigator for young children such or a Nose Frida for babies and toddlers too young to blow their nose.
- Complete recovery takes about a week after fever onset. If measles is treated early using nutritional and natural wellness approaches, it is important to note that rash can be mild or even non-occurring.
- If fever gets uncontrollably high or you are concerned about your child’s well being, seek emergency care.
- If your child is exposed to measles and you would like to explore pharmaceutical intervention through immune globulin or post-exposure MMR see the CDC discussion of this under the section “Post-exposure Prophylaxis”.
I also was amused at the lack of urgent reaction to this question posed on the “measles frequently asked questions” page on the CDC website which actually gives instructions for measles home care:
From the CDC measles FAQ page:
Q: My doctor or someone from the health department told me that I have measles. What should I do?
A: If you have measles, you should stay home for four days after you develop the rash. Staying home is an important way to not spread measles to other people. Talk to your doctor to discuss when it is safe to return.
You should also:
- Cover your mouth and nose with a tissue when you cough or sneeze, and put your used tissue in the trash can. If you don’t have a tissue, cough or sneeze into your upper sleeve or elbow, not your hands.
- Wash your hands often with soap and water.
- Avoid sharing drinks or eating utensils.
- Disinfect frequently touched surfaces, such as toys, doorknobs, tables, counters.
Call your doctor is you are concerned about your symptoms.
——————————-
Did anyone find this completely void of any urgency like we are so often taught is needed regarding measles? And did they really need to tell us how to use a tissue? 😉
I also think it would have been nice to include a little bit of advice on how to CARE for measles. There is absolutely no strategy offered for boosting the immune system, supplementing for nutritional deficiency (Vitamin A), hydration, or self-care. Strategies that are supported by dozens of studies supporting a better outcome with measles.

My Thoughts:
Several years back, after the Disneyland measles “outbreak” of 2015, I found myself negatively affected by the media and my confidence in our decision to forgo the MMR was bruised. I am more confident today thanks to spending the time to publish my research and share it publicly, but it can still be frustrating to be labeled simply as an “anti-vaxxer” when we studiously considered each vaccine and learned about each disease. We are NOT anti-vaccine, we are pro-RESEARCH and ultimately pro-choice.
When we decided to delay and then eventually forgo vaccines, my husband and I were incredibly intentional about where the greatest risks were for disease exposure. As you read in my other vaccine posts, even after my husband lost his job in 2009 and we were living off of my teacher’s salary, we worked opposite shifts so one of us could be home with our first daughter after she was born.
We stayed home from school and church when any of us were sick, ate a mostly organic and high plant-based diet, and invested each month in supplements we knew were studied to show increased immune cell activity such as Beta-1, 3D Glucan, appropriately strained probiotics, and a food-based vitamin. I also breastfed (or pumped for) all of our children for 12-18 months.
When our kids are small and their immune systems are still developing we take precautions in public places by choosing outdoor environments, washing hands as soon as we get home, and covering the baby carrier in less-ventilated places like in an elevator or a small room. We even attended church in the evening, a less popular time for large amounts of kids in one room, reducing our risk. When we did require childcare for several years before I was able to stay home with our kids, we chose a small home-based day care.
This is not to say we are hermits- our children still attend normal activities as they get older and their immune systems are more developed. They go to the children’s environment at church, gymnastics class, ballet, the gym daycare once they’re over 9 months, and eventually public school, where we have started our oldest when she reached 2nd grade. An often ignored benefit of homeschooling until 2nd grade was healthy SLEEP. I find that keeping them all home and allowing them to sleep until they wake up each day is also a contributing part of them staying so healthy all of these years.
Over nine years later, we have four unvaccinated kids who are healthy, bright, and have never had or taken an antibiotic (or any pharmaceuticals) for today’s common childhood maladies such as ear infections, strep throat, hand foot and mouth disease, sinus infections, bronchitis, or had autoimmune issues, allergies or asthma. We have been fortunate enough to have had success caring for them at home and have avoided the doctor’s’ office in this time span altogether. They have also never had the measles, something I am prepared for if they were to.
My Grandmother’s Wisdom:
While I was on a routine call with my 93-year-old amazing grandmother one day, I decided I wanted her perspective on measles and felt blessed that she was still around and had such a superhero memory to answer my questions!
Our conversation went like this:
Me: “Grandma, can I ask you something about measles.”
Grandma: “Sure. (chuckling) Why are you asking about measles (chuckling)?”
Me: “So, did you or any of your kids have measles back in the day?”
Grandma: “Everyone got the measles back then. When your father was in grade school he got it and I sent the rest of the kids to sleep in his room so they would all get it at the same time and we could get it over with!”
Me: <shocked> “REALLY??? <still shocked> Did any of them get really, really sick?”
Grandma: “Fevers could get pretty high but it was similar to a bad cold with a rash. Just kept them inside resting and drinking lots of liquids. It passed in a week and you never had to deal with it again.”
I couldn’t believe that was all she had to say about it.
She completely under-reacted and even chuckled at my prompting! It is right in line with the video I mentioned above.
Our ability as parents to recognize symptoms and keep our children home, perform basic at-home care, know how to manage fevers, properly remove mucus and drainage from our children, and understand when to seek emergency care is essential if a measles infection were to occur.
My conversation with my grandmother also got me thinking of all of the nutritional, medical, and therapeutic resources and knowledge we have today compared to the 1960’s if measles complications did occur (see treatment section above.) Natural remedies can be delivered to our doorstep overnight and emergency care is readily available if needed.
Even though most babies are born to vaccinated mothers today (like myself) and therefore have lower antibody protection (see studies above), significantly more babies are breastfed today, resulting in better equipped immune systems with more protection than formula fed counterparts. In the 1950’s and 60’s it was advised best (and was a status symbol) to give babies formula and yet death from measles was a rarity.
Study after study has confirmed that proper nutrition and hygiene has everything to do with positive measles outcome (if not all disease outcome.) Comparing impoverished areas in other countries to the U.S. is comparing apples to oranges, but global statistics are often the only ones brought up by the media when reporting about the death rates and severity of measles.
Addressing the Protection of Immunocompromised Children:
“But what about kids with cancer, the immunocompromised or babies that can’t be vaccinated?”
A common argument amongst the public and presented in the media is about the need to vaccinate the healthy “herd” in order to protect kids too young to be vaccinated or the immunocompromised, such as people with cancer going through chemotherapy.
I already addressed the concern about healthy younger babies above, but the truth of the matter regarding cancer patients is complicated. Kids going though chemotherapy or who have an immune system condition shouldn’t be around germ infested places like schools and daycares and jumpy house places anyways.
It is a season where these environments would be unsafe, regardless of vaccination status. Even kids who have received all of their vaccines get sick with hundreds of other diseases that aren’t on the vaccine schedule (and even with ones that actually are such as whooping cough, rubella, flu, rotavirus, and chickenpox which they can actually shed and spread to others, too.)
This is why you will often see signs in cancer centers or hospitals about not visiting if you have recently been vaccinated with the live flu or chickenpox vaccines.
From MMRV insert: “Vaccine recipients should attempt to avoid, to the extent possible, close association with high-risk individuals susceptible to varicella (chickenpox) for up to 6 weeks following vaccination. In circumstances where contact with high-risk individuals susceptible to varicella is unavoidable, the potential risk of transmission of the varicella vaccine virus should be weighed against the risk of acquiring and transmitting wild-type varicella virus.”
Many cancer treatment centers will actually recommend that patients get any vaccines they may “need” before their treatment starts. Here’s a sample of the recommended vaccines and their time-frame before chemotherapy from MD Anderson. Although the MMR cannot be given during treatment- the MMR insert states that “patients with leukemia in remission who have not received chemotherapy for at least 3 months may receive live virus vaccines. Short-term (<2 weeks), low- to moderate-dose systemic corticosteroid therapy, topical steroid therapy (e.g. nasal, skin), long-term alternate-day treatment with low to moderate doses of short-acting systemic steroid, and intra-articular, bursal, or tendon injection of corticosteroids are not immunosuppressive in their usual doses and do not contraindicate the administration of [measles, mumps, or rubella vaccine].”
This leaves a very small percentage of patients who could not receive a vaccine (who was not already old enough before their cancer to receive an initial dose or both doses of MMR.)
And for the record- if my child is exhibiting ANY symptoms of illness (runny nose, cough, fever, etc) or has recently had ANY of that, or even if it is just cold and flu season, I am not going to bring them into a hospital setting, to see a friend with a young baby, or visit an elderly relative regardless of their vaccination status. I may consider not even bringing them into such a vulnerable place at all just as a precaution.
Respectful human being / common sense kind of stuff there. 🙂
****Make sure to visit my MMR Vaccine post to see specifically why this vaccine concerned us and the data that proved that this vaccine is NOT 100% safe nor effective. You can check that post out HERE.****
