

Before the birth of our first child and prior to starting my research on vaccines, this is about how much I thought I knew about polio and the polio vaccine:
- Polio was a really big problem before the vaccine.
- Lots of people were paralyzed from polio before the vaccine and many died.
- After the vaccine everyone was saved from polio! The end.
It’s not quite that simple though. And I think it’s so important for parents evaluating this vaccine to know the big picture around the rise of polio and all of the factors going on at the time just before and after its peak.
The process of writing this post about polio and the polio vaccine was incredibly intense. At times I just wanted to give up this entire series on vaccines because research on polio was difficult and puzzling. Whereas my other posts on vaccines took a few weeks of compilation and research, this post took months. I’m a huge proponent of “doing hard things”, but when it comes to the history and science and statistics of polio, there is just SO MUCH.
So much history, so much varying opinion, so much politics, and so much FEAR. It’s taken a lot of time to detangle the story and break it down to you guys in a way I think makes sense and stays factual.
To complicate the story even more, just as I was about to wrap up my research on this post, a bombshell was dropped on everything I thought I believed about polio. I found out that my own DAD had polio when he was a toddler. I’m not sure how this never came up in conversation, seeing how big of a deal it is in our culture. But my family never mentioned it.
Last night I had an excellent talk with my 93-year-old grandmother about what it was like going through a polio diagnosis with her child. I knew I had to talk it through with her before I published this post, and what she said cemented my confidence in my decision about polio vaccination even more.

This is Part 4 in my vaccine series discussing how we made our decision on which vaccines to give our children. You may also want to check out the other posts in this series:
Part 1: Our Vaccine Choice: Risks, Benefits, Responsibility
Part 2: Hepatitis B and Hib Vaccines
Part 3: Diphtheria, Tetanus and Pertussis Vaccine
Part 4: Polio
Polio Symptoms:
- fever
- sore throat
- nausea and vomiting
- muscle weakness
- pain and stiffness in neck or back
- paralysis
Overview: (CDC)
Poliomyelitis or polio is a transient virus of the gastrointestinal tract. It enters the body through the mouth and can colonize in the pharynx (throat) or in the gastrointestinal tract. There are three poliovirus serotypes, P1, P2, and P3. The virus can invade the lymph tissue, bloodstream, and then in less than 1% of cases it can travel to the central nervous system where permanent paralysis can occur. The virus is excreted from the bowels and can be found in stool up to three weeks after infection.
- Incubation period for polio is 3-6 days with paralysis (<5% of cases) occurring usually 7-14 days after exposure.
- Polio is spread through oral ingestion of microscopic fecal matter usually through contaminated water or food. It is less commonly spread through oral or nasal secretions.
- Polio typically circulates through communities in the summer months.
- Approximately 72% of polio cases have no symptoms. Another 24% infected with polio have minor symptoms such as low grade fever and sore throat. This is a total of 96% of total polio cases without any paralysis or major illness with complete recovery in less than a week.
- 1-4% of those infected with polio have temporary paralysis lasting up to 10 days where after complete recovery occurs.
- Less than 1% of people affected by polio maintain a state of paralysis for more than ten days and have ongoing effects from paralysis. (1 in every 200 infected people)
Timeline: Rise of Polio and the Polio Vaccine Campaign
Polio cases significantly rose from a rare illness of mild symptoms in the 1800’s to an alarming and mind-boggling disease in the mid-20th century. Its rise coincided with many of our national industrial, cultural, and military milestones that I think are important to look at as well.
Once I started wondering about the statistics and the mysterious rise of polio in the 1950’s, I began to look for connections with what was going on in our country at the time. My research ended with me leaning more towards “puzzled” than fearful. There was plenty of information that just didn’t add up with what we are commonly told about polio and its eradication.
- Pre-1900: I have had such a hard time finding information or statistics about polio in the 19th century or earlier. It was a rare and mild disease that wasn’t for much concern from a public health perspective. In some states, such as Connecticut, polio was so rare it wasn’t even a reported disease until 1921. I could find very little to no 19th century data on polio like I could for the other diseases in this vaccine series.
- 1890’s-1920’s: During the late 1800’s and early 1900’s cities significantly cleaned up with community sanitation efforts, indoor plumbing, sanitized water supply, and sanitation efforts in hospitals. The most popular mainstream theory for the rise of polio is related to this which I’ll go into later in this post.
- In 1916 in New York City over 6,000 people died from complications with polio and many were paralyzed. There were 27,000 total paralytic cases and most of the effect of this was felt in the large metropolitan areas of New York City and the mid-Atlantic. There is a strange connection to the area of the initial breakouts in New York City in poorer immigrant neighborhoods in Brooklyn and the location of the Rockefeller-funded research lab where research was being conducted on a strain of monkey polio virus. It is well documented that the 1916 polio strain was unlike typical wild polio in its severity and ability to spread. Nothing like it has been seen since.
- During the years of World War I (1914-1917), the Great Depression (1929-1940), and World War II (1941-1945), the use of chemicals and dumping of toxic waste with unknown consequences at the time, were of great un-concern because of American war and recovery efforts. So much of what we know now about toxicity when it comes to chemical waste exposure was not applied then as it is now. Studies were still being performed to figure out what was causing this mysterious paralysis, eventually landing on the viral-only theory.

1900-1960’s: Breastfeeding decreases significantly as cows’ milk use and formula production and mass distribution becomes a social status consideration as well as easier for mothers in the workforce (reducing protective antibody exposure to infants.) By 1930, commercial formula takes over the use of both cow’s milk supplementation and breastfeeding. By 1950 breastfeeding is seen as socially unacceptable and an option for the poor or done in secrecy. Although I could not find any scientific literature studying the relationship between breastfeeding rates dropping, cows’ milk use and formula use with polio rates, I can imagine just from looking at the the sanitation theory of polio and how maternal antibodies were the key to protecting children from wild polio virus exposure, that DECREASED breastfeeding rates would result in DECREASED maternal antibody protection. Again- just my thoughts and I have NO IDEA why this hasn’t been addressed or studied!
- 1945-1951: Polio case rates double from 19,000 in 1945 to over 40,000 in 1950.
- October, 1951: Dr. Albert Sabin publishes the sanitation theory of polio in The American Journal of Public Health after studying indigenous populations low occurrence of paralytic polio vs. westernized cultures. He hypothesizes that infants exposed to polio earlier in life through fecal contamination develop asymptomatic, lifelong immunity to polio. And since they are still protected by maternal antibodies when exposed, they don’t have symptoms nor suffer paralysis. When exposure is delayed in more developed cultures with advanced sanitation, polio infection occurs later when maternal protection is no longer present.
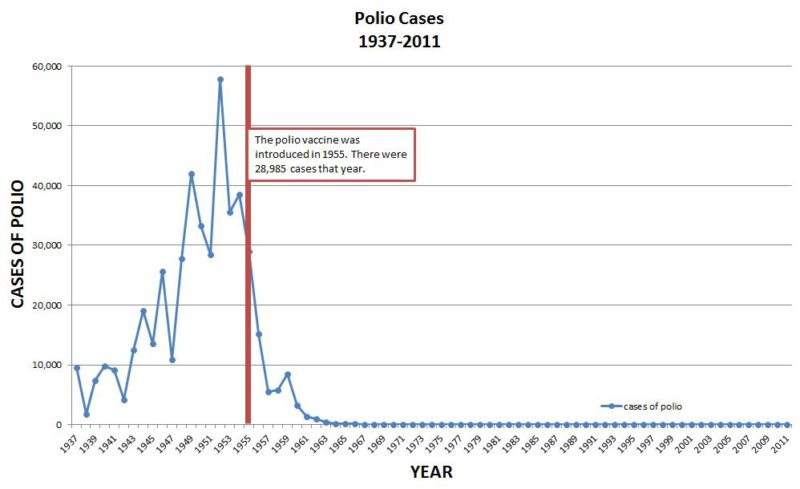
- 1952: Polio rates in the U.S. gradually rise reaching a high of 58,000 cases (both paralytic and non-paralytic combined.)
- 1953: 36,000 cases of polio in U.S. Dr. Jonas Salk announces 90% successful injectable polio vaccine.
- 1955: Salk Vaccine (IPV) in widespread use in the U.S. Polio rates drops to 29,000 cases (both paralytic and non-paralytic combined.)
- April, 1955: More than 200,000 children receive the IPV (Salk) polio vaccine that did not use a proper amount of formaldehyde and left active polio virus to take hold, causing hundreds to thousands of cases of paralytic polio and killing 10. This came to be known as the Cutter Incident.
- Late 1955: Diagnosis criteria of polio is changed automatically reducing polio cases by up to 60% to only paralytic polio cases. (see discussion below.)
- 1956-1960: Polio cases drop to ~5,000 cases annually after diagnosis criteria changes, eliminating paralytic cases lasting under 60 days (only paralytic polio now recorded as a polio case.)
- 1961: Dr. Sabin’s Oral Polio Vaccine (OPV) goes into widespread use in the U.S, especially in schools where children receive their polio vaccine dose on a sugar cube.
- 1962: Discovery that some IPV (Salk) vaccines used from 1955-1963 were contaminated with simian virus 40 (SV40) from the monkey culture used to produce the vaccine. As many as 100 million people injected with SV40 contaminated vaccine. People who received a contaminated vaccine have an increased risk of cancer. We have since then learned that SV40 can also can be passed down to next generations through the mother.
- 1979: wild polio considered eradicated from the U.S
- 2000 – today: OPV discontinued in U.S due to live virus “VAPP” or vaccine associated paralytic polio. Injectable IPV takes its place as the standard vaccine. OPV is still the most affordable and widely used polio vaccine used overseas in countries targeted for eradication which continues today.
Other Factors Considered in Polio Incidence:
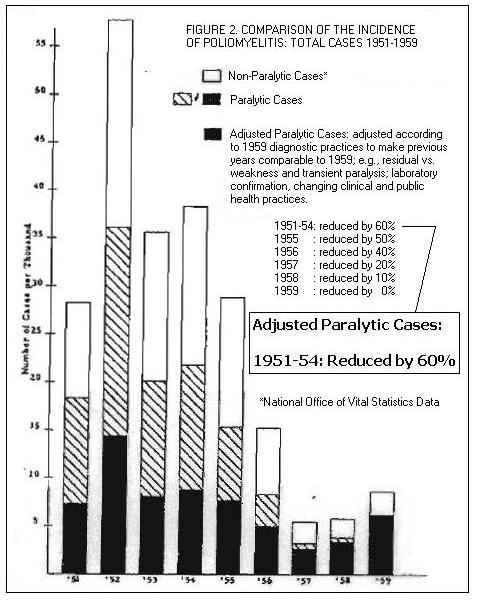
COMPARISONS OF POLIOMYELITIS 1951-1959
Reclassification of Polio to Only Long Term Paralytic Cases:
Before 1954 and before the vaccine, polio was diagnosed when a patient had “partial or complete paralysis of one or more muscle groups, detected on two examinations at least 24 hours apart.” These are WHO recommendations. So, basically, when any kind of muscle weakness or paralysis occurred in you or your child, you saw a doctor who noted you have muscle weakness of some sorts and flagged you for possible polio infection. Then 24 hours later you returned to the doctor and if you still had symptoms of weakness or paralysis- BAM- a polio diagnosis. This would amount for a whole lot of cases of polio- which is what we saw in the mid 1940’s to mid 1950’s.
In 1955, after the Salk vaccine campaign was in full effect, the official diagnosis criteria CHANGED and the patient had to have paralytic symptoms at the initial doctor visit and then instead of 24 hours later, they had to now have paralysis at least 20 and then 60 days later to be a confirmed case! This eliminated anyone whose symptoms went away between days 2 and 59, and with it a ton of polio cases! Even vaccine researchers admit <— (see page 2) that this is automatically a lot of polio cases GONE with or without the vaccine. You would no longer be a case on the graph if your symptoms went away before 60 days.
In order to qualify for classification as paralytic poliomyelitis, the patient had to exhibit paralytic symptoms for at least 60 days after the onset of the disease. Prior to 1954, the patient had to exhibit paralytic symptoms for only 24 hours. Laboratory confirmation and the presence of residual paralysis were not required. After 1954, residual paralysis was determined 10 to 20 days and again 50 to 70 days after the onset of the disease. This change in definition meant that in 1955 we started reporting a new disease, namely, paralytic poliomyelitis with a longer lasting paralysis.
-Dr. Bernard Greenberg, head of the Department of Biostatistics of the University of North Carolina School of Public Health
The graph above is a helpful visual to digest what I’m talking about. The areas with the striped bar are cases of polio that would not have been classified as polio under 1954 criteria bringing a much less dramatic reduction of polio cases to the table.
After 1958 there was a new push to separate paralytic polio cases from other paralysis-causing diseases such as transverse myelitis, aseptic meningitis, Guillain-Barre syndrome, chronic fatigue syndrome, spinal meningitis, Reye’s syndrome, and several others including acute flaccid paralysis. Before this effort, these would all have been classified under the “polio” umbrella of disease.
By 1960, polio cases could only be diagnosed by confirmed stool sample from a laboratory, creating even more strict criteria and less polio cases.
Environmental Factors and Chemical Usage:
The graph above really paints a well-rounded picture of what was going on around the time of increased polio incidence in the U.S.
The amount of back and forth between different experts disagreeing about the relationship of chemical use and polio made my head spin at times. It is sensical that with increased industry and chemical usage on crops and in our water and dairy supply after World War II, problems would occur. Whether polio is one of these problems is debatable but in the early 1950’s Dr. Morton S. Biskind studied the topic thoroughly and was widely dismissed and shunned by a medical culture entrenched in the viral-only theory of polio.
He says:
“Since the last war there have been a number of curious changes in the incidence of certain ailments and the development of new syndromes never before observed. A most significant feature of this situation is that both man and all his domestic animals have simultaneously been affected. In man, the incidence of poliomyelitis has risen sharply…
“When the population is exposed to a chemical agent (DDT) known to produce in animals lesions in the spinal cord resembling those in human polio, and thereafter the latter disease increases sharply in incidence and maintains its epidemic character year after year, is it unreasonable to suspect an etiologic relationship?”
You can see in the below graph the work of the Weston A. Price Foundation comparing DDT chemical use in the U.S to the incidence of polio. The article it accompanies is excellent and includes many other sources in its bibliography. You could easily study this topic for years.
Source: westonaprice.org
I tend to lean towards an environmental influence on the invasive nature of paralytic polio incidence due to chemicals such as DDT and the arsenic-lead compounds that came before it. Whether it affected us by altering our gut biome allowing for polio virus to access the central nervous system more easily, or if it was simply direct poisoning is discussed in much of the scientific literature on the topic of DDT and other insecticides and polio incidence.
Many of the generation born in the 1940’s and 1950’s remember the DDT trucks circulating neighborhoods spraying lawns, trees and swimming pools in the summertime to kill mosquitoes (also the time when polio surged each year.) Some remember even playing in the spray as the trucks rode by. In India where cases of acute flaccid paralysis (a renamed version of polio symptoms) is on the rise today, DDT is still sprayed several times a year.

DDT being sprayed in pool, 1950’s
Injection-Induced Polio (Provocation Polio):
There have been several studies done on the link between paralytic polio infection and the rise of pertussis vaccination in the late 1940’s and then with widespread polio vaccination in the 1950’s. The idea is that by getting an injection into the muscle (most likely the DTP vaccine) while having active, but most likely asymptomatic polio- invasion of the central nervous system can occur leading to paralytic polio.
A 1998 study was able to reproduce this effect in mice:
“Muscle injury due to injection of vaccines or therapeutic agents is common in medical practice. It has been observed that, if concurrent with PV infection, such injury may increase the risk of neurological complications…we have shown that muscular trauma induced by multiple injections can lead to rapid progression of PV-induced paralysis”
You can also read more in these studies on injection-induced polio:
The Relation Between Injections and Poliomyelitis in Children

Tonsillectomies:
I’m including the theory of excessive tonsillectomies in with this discussion because of a significant amount of study and research done in relating polio incidence in children and adults who received a tonsillectomy in the 1940’s and 1950’s.
Tonsillectomies were the most common medical procedure performed in the U.S. from 1900-1965. In 1959 alone 1.4 million tonsillectomies were performed, mostly in middle to upper class children.
The concern was not so much that these children were more prone to polio infection, but that they had a significantly higher rate of developing bulbar polio, the kind that had the worst forms of paralysis and affected your lungs. These patients were the rarest of polio infection and were the ones you see in the pictures of the iron lung wards. (see above)
In one study of a Utah 1943 polio outbreak, it was found that 43% of the children with bulbar paralytic polio had a tonsillectomy performed within 30 days of the onset.
Dr. Albert Sabin, creator of the oral polio virus (OPV) vaccine even studied and took note of this.
For additional reading on this, you can check out:
American Journal of Public Health, 1954: Tonsillectomy and Poliomyelitis
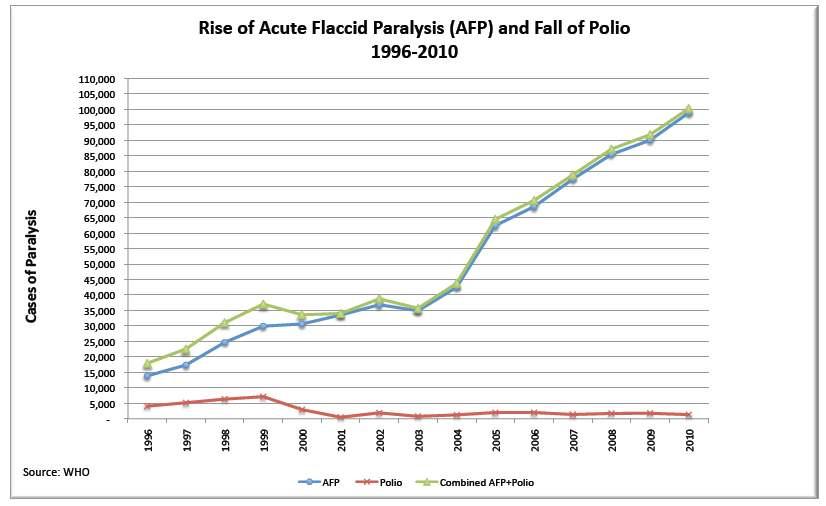
AFP in the U.S. and in India:
When evaluating polio and the polio vaccine, this last point is so important to reinforce. Polio was reclassified and all non-paralytic cases of polio were thrown away with the change in 1954. This dropped the data overnight. With it came new diseases and the acknowledgement of old diseases.
There are many other viruses and conditions that cause temporary to permanent paralysis that are seen still today and documented in the early 20th century including Coxsackie virus, aseptic meningitis, Guillain Barre Syndrome, transverse myelitis, certain enteroviruses, and acute flaccid myelitis, amongst many others. In 2015 alone over 3,000 cases of acute flaccid myelitis were diagnosed in our country. CNN even surprisingly reported about it! Coincidentally, acute flaccid myelitis also peaks in summer and lessens in winter just like polio. Another name for acute flaccid myelitis is “Acute Flaccid Paralysis” which we often hear when referring to India’s paralysis problem that is magically not polio- but has risen since the “eradication” of polio in India since the early 1990’s.
In the 1950’s many of these would have been classified as “polio.”
See below.
Polio Vaccine Information: (CDC)
Vaccine Ingredients:
IPV (Salk inactivated polio vaccine- used in the U.S. – injectable)
- All three inactivated strains of poliovirus
- M-199 culture medium made from saline, vitamins, amino acids, sucrose, glutamate, monkey kidney cells, and human albumin
- 2-phenoxyethanol- about 0.5% of the solution
- Formaldehyde (about 0.02% of the solution)
- Residual amounts of antibiotics
- Traces of calf serum
According to the CDC, the IPV gives 90% or more immunity after 2 doses and at least 99% immune after 3 doses. Duration of immunity not known with certainty.
OPV (Sabin oral polio vaccine- used overseas, discontinued from use in the U.S. in 2000 due to risk of shedding in stool) For ingredients and information see the CDC Pink Book.
It’s important to note that this vaccine is often given in combination with other vaccines at 2, 4, and 6 months.
VAERS reported 657 adverse reactions in the U.S. from the IPV, inactivated polio vaccine and combo vaccines with 2 reported deaths after vaccination in 2016.
VAERS reports have the potential to be a great tool for transparency in vaccine research, but unfortunately data there is significantly underreported. Many vaccine injuries are cumulative and have slow or gradual onset and go unnoticed until it is serious later on. Also, VAERS reports are volunteer-based so it relies on doctors spending their time filling out vaccine injury reports or parents doing it themselves (even though many parents don’t even know it is there to use). Because of this, there is increasing popular belief that vaccine injuries are most likely 10 to 100 times higher than what is actually reported in VAERS.
Emergency Care:
Obviously the chances of developing paralytic polio in our country are extremely rare, but if you suspected your child had paralytic polio, seeing a practitioner that is versed in emergency care for polio would be essential. Having a plan ahead of time and discussing this with your practitioner is important.
In the U.S. a case of polio in an unvaccinated child would be headline news. Choosing to treat a child at home with herbs, nutrition, and home care would realistically- probably end us up in jail. So talking to a trusted practitioner who is supportive of your vaccination decision ahead of time would be a responsible move and would give you more peace. Again though, unless you travel internationally often, chances of polio infection is incredibly low.
I definitely wonder if polio would have been an issue in the early 20th century if people back then knew what we know now about chemical exposure, nutrition, and the importance of breastfeeding for antibody protection against polio.
Consumption of organic fruits and vegetables not sprayed with chemicals, cultured and fermented food on a weekly basis and daily probiotic to protect gut health (as a compromised gut could increase likelihood of nervous system involvement) are important in prevention of paralytic polio.
If infection is suspected, early intervention of high dose Vitamin C therapy, nutritional nourishment, and antiviral herbal remedies such as elderberry and astragalus, osha, and echinacea as glycerites can prevent occurrence of paralytic polio. (Source)
I personally would make sure my child was sufficient in B vitamins, selenium, Vitamin D3/K2 and magnesium which will help relax the nervous system.
Homeopathic remedies and homeoprophylaxis (although discredited and dismissed by mainstream medicine) have shown to be effective towards polio in smaller populations studies. You can read more about that HERE.
Thankfully, the old practices of isolation of muscles in cases of paralysis were already losing popularity to the physical therapy methods taught by Sister Kenny in the 1950’s.
My Thoughts:
My Dad’s Polio Story
As I mentioned above, just as I was about to publish this post, I found out from my dad that HE HAD POLIO as a toddler. He knew very little details about it so I called my 93-year-old grandmother to get the facts. She was able to recall the entire situation like it was yesterday.
She told me that when my dad was born he was a very sickly child. I asked her about his birth and she said she labored for a bit and then they gave her a shot in the hospital and she passed out and doesn’t remember the rest but he was delivered normally after using “the tools that help get the baby out.” They took my dad from her immediately after she held him for the first time. She said she wanted to nurse him but the doctor told her that her milk was too rich so they put him on Carnation formula in a can. She said they discovered that his bowel was obstructed at birth and it caused a lot of problems. He lost 3 pounds in two weeks and the doctors didn’t think he would make it. “He was a miracle.” She said he began to tolerate the formula better but as he got older he could only eat foods that were plain and no citrus foods or rich foods as they would cause him to have stomach problems.
Around his first birthday he started walking. Shortly afterwards “he got sick and then couldn’t get up to walk and his legs were very weak.” The pediatrician sent them to the children’s hospital in Detroit and there they taught my grandparents “Sister Kenny’s physical therapy” that they did for several weeks at home until his legs were strong enough to walk again.
My grandmother also mentioned that the house they lived in had no indoor bathroom and they had an outhouse with a septic tank. She and my grandfather had bought a “house shell” for $3,000 and were gradually saving up to add a completed bathroom and kitchen. They even installed their own electricity and plumbing with the help of their parents and siblings! 1948 was such a different time than how we live today.
Looking back at my dad’s story, I wonder how different it would have been if he would have entered the world today with what we know about disease prevention and avoiding unnecessary medical intervention. What if he would have received maternal antibody protection from polio through breastfeeding, had an indoor toilet in their home, and had appropriate care for his bowel obstruction? Just like with tonsillectomies and with the polio-injection provocation theory, could it have been my dad’s bowel obstruction and gut problems created a pathway for polio to gain access to the central nervous system? I find myself being incredibly grateful he was able to receive appropriate physical therapy and my grandparents were mindful for how to care for him. So many others didn’t have this option or information.
Our Decision:
Deciding on whether to give the polio vaccine was a difficult decision to make. The public health aspect is important to me and the IPV has been in use for over 40 years in the U.S. and is considered the “safest” of the vaccines due to its seemingly low side-effect profile.
Even with that information, my husband and I were still not comfortable with the idea of bypassing our daughter’s natural defense barriers and injecting a foreign substance into her bloodstream so early in life. The ingredients in the vaccine are also concerning. There is still so much to learn about the cumulative effects and role in chronic disease and cancer in relation to vaccination.
With all that I learned about the entire history of polio in the U.S. I felt that so much of what was causing the polio problem and vulnerability towards paralytic polio in the early 20th century were things we have already corrected from past generations (with high plant-based organic diet, focus on gut health, unmedicated childbirth, exclusive breastfeeding, hand washing, knowledge of supplemental nutrition, etc.)
Since we would not be traveling outside of the U.S. to at-risk areas, our daughter was exclusively given breast milk and was cared for at home, and we became knowledgeable about polio risk factors, symptoms and options for care and treatment, we have chosen to DELAY polio vaccination indefinitely.
We understand that the risk for polio infection in the U.S. is significantly low and have many reasons to believe (as discussed above) that other factors such as exposure to pesticides and insecticides, unnecessary tonsillectomies, nutritional deficiencies and availability of emergency care and appropriate physical therapy for paralysis early on- could possibly alter disease outcome.
If she goes into the medical or mission field or travels to polio-prone areas as an adult, we will discuss the risk with her of polio where she is traveling and discuss with our holistically-minded MD and homeopath before making a decision on vaccination. If a vaccine for polio is ever necessary and given in the future, we would follow up with an appropriate detoxification protocol.
Any thoughts on polio or the polio vaccine? I’d love to chat with you. Leave your comments below! 😀

Thank you so much for all of your research and information! My wife, newborn, and I live in Lilburn, GA and it has been tough finding a pediatrician that does not mandate strict adherence to the vax schedule (we found one, thank the Lord). Do you have any input regarding these new combination vaccines, such as Pentacel (Hon, TDaP, and Polio)? Thank you
Did you give your daughter any vaccines at all I keep pushing my babies back he just turned 4 months
We didn’t give any. In each post towards the end, I give a summary of our decision. 🤗
Wow. Very good article. Thanks for doing all this research. I have relatives who are not giving their children vaccines – so this information is enlightening.
You’re welcome, Valerie!
I have known a couple of people who had polio as children. As they reached their 50’s – 60’s, they got post-polio syndrome. I’m stretching my brain a bit so maybe I am thinking of a different disease. But I don’t think so. Did you read anything about that in your studies? Like chicken pox causing shingles later in life. It’s just another consideration regarding vaccination.
It amazes me how much research you go through! I guess that is why I trust what you write. Thank you so much!
Hi Jeanne, no you are totally spot on. Post-polio Syndrome is a real thing that people deal with about 35-40 years after their initial bout. I didn’t dig in to it in great depth but I know there are support groups for people that are going through it.
So with all of the mandates are you having to homeschool your kids?
We have always homeschooled but my oldest went to a public charter for two years and we used the religious exemption which Georgia still has.
Excellent information. Thank you for sharing all your hard work.
Wow! Thank you for all the good research and information. That is an eyeopener. Was already wary of vaccines, but polio? Indoctrination leads us to believe polio just might be worth it. The corruption in this broken world is mind boggling.
Absolutely one of the best articles I’ve read on the subject!! I’ve read a lot of good articles but usually they are too simple and mostly opinion or too detailed to pass on. This hit the nail square on the head!
And I’m thankful your dad’s doctor knew about Sistey Kenny! What a blessing! The story might have ended differently otherwise.
Thank you for all your research and clarity. Keep up the good work. 👍🏻💐
Excellent research and very informative! Thank you, Cortney.